The Neuroscience of ADHD
ADHD: Myth, Medical Condition, or Something More Nuanced?
“ADHD was invented as an excuse for parents to give boys drugs to make them sit still,” or such was the wisdom of my middle school social studies teacher. I heard some version of this from sundry parents, teachers, and even students over the course of my childhood. The enemy was a restrictive education system, impatient teachers, strict parenting, lax parenting, food preservatives, television, video games, or some combination depending on the moment.
More recently, high profile publications like The Chronicle of Higher Education and The Atlantic have published articles suggesting that too many students in higher education are receiving disability accommodations. The culprit, they suggest, is a deluge of wealthy parents seeking diagnoses from unscrupulous practitioners. At the same time, the Make America Healthy Again report released in May cites concerns about “overuse of medications in school-age children” and inappropriate diagnostic thresholds for ADHD.
ADHD excites controversy in a way that few other diagnoses do. No one is out there arguing over whether too many kids are allowed to wear glasses nowadays (although rates of myopia are on the rise).
Perhaps some of the ADHD skepticism arises from the murky biological basis of a diagnosis that relies on behavioral differences in functions as abstract as attention and self-regulation. It should come as no surprise that the biological underpinnings of ADHD are complex, considering that attention itself is a process so complex that it remains an area of active research.
The consensus among neuroscientists is that while ADHD has a well-established basis in genetics and neurology, this basis is multifactorial, meaning that there is no single gene or mechanism that causes ADHD. Instead, ADHD is caused by a confluence of biological variables that differ between individuals with the same diagnosis.
Abandoning the Monolith: in search of new models for ADHD
A growing body of research explores how ADHD might emerge because of differences in a variety of neural pathways, or circuits, between different brain regions. To make things a little more concrete, I’m going to dive into a model of ADHD theorized by Dr. Sarah Durston and colleagues in a 2011 review. I’ve chosen this model to discuss, not because it represents the final word on ADHD research, but because it presents a clearly articulated model that synthesizes a variety of findings in ADHD research. Durston and colleagues conceptualize ADHD as arising from differences in three related but distinct brain circuits, all of which involve the prefrontal cortex as a key participant. This model builds off of prior work conceptualizing ADHD as a difference in prefrontal cortex function but takes a more wholistic approach that helps explain how ADHD might manifest differently in different people.
The Cognitive Control Circuit
Switching tasks, suppressing impulses, and managing attention all fall under the broader umbrella of cognitive control, a function managed by the prefrontal cortex in concert with the C-shaped dorsal striatum and the brain’s central processing hub, known as the thalamus. Specifically, neurons in the pre-frontal cortex send electrical signals to the dorsal striatum, a brain region involved in planning and selecting appropriate behaviors, and parts of the thalamus known to be involved in executive function.
Durston and colleagues report that unpublished data from their lab show microstructural differences in the connections from prefrontal cortex to striatum in children with ADHD compared to their neurotypical peers.
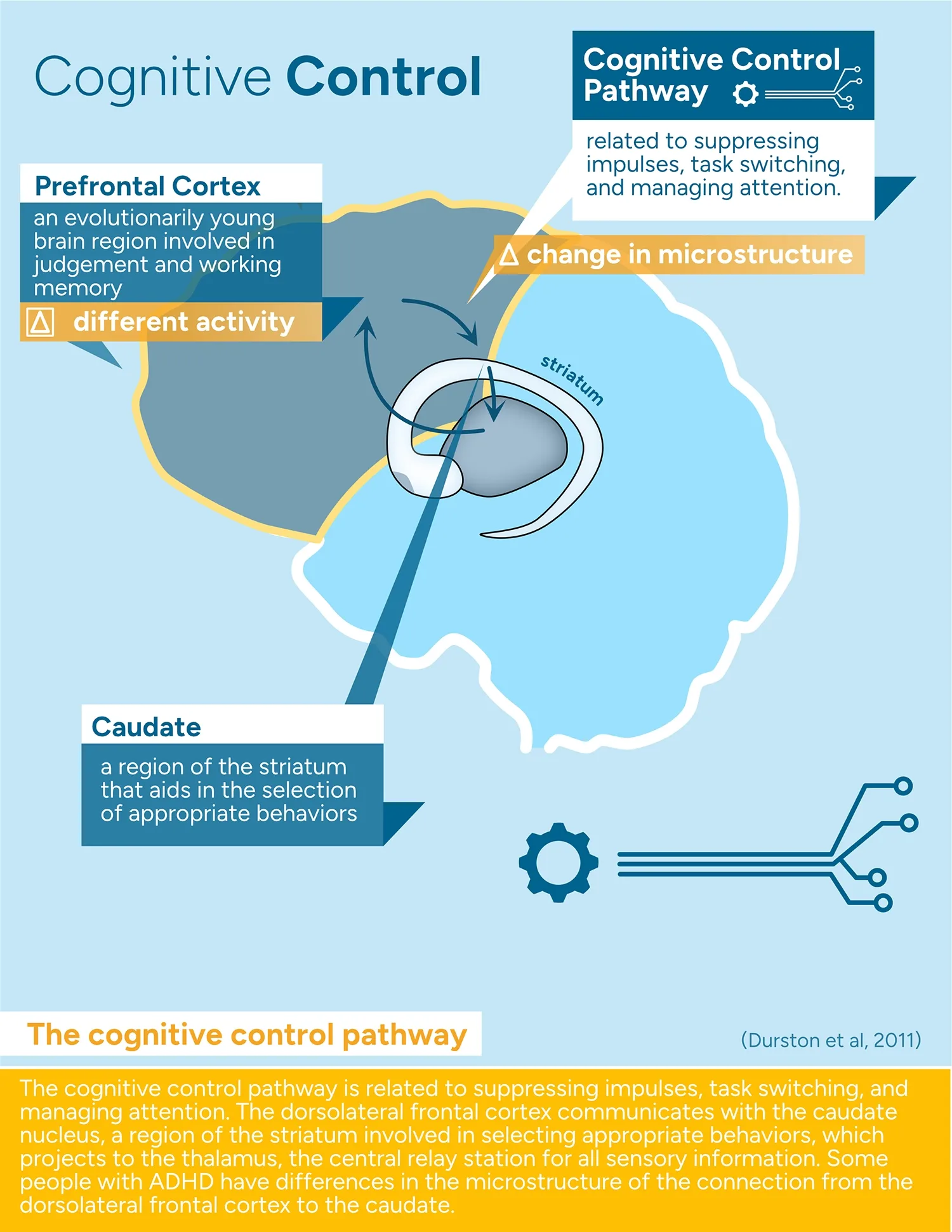
Key takeaway: The prefrontal cortex and the dorsal striatum work together to support “cognitive control,” a similar concept to executive function. Preliminary evidence shows that children with ADHD might have microstructural differences in the neural connections between prefrontal cortex and striatum.
The Reward Circuit
Everyone who has had a passing interest in ADHD biology (and many who haven’t) have heard dopamine referenced. Content about dopamine hits and dopamine hacks flood social media. Dopamine, it seems, is the ultimate feel-good molecule.
Dopamine, for all the hype, is just a molecule that acts in different ways in different parts of the brain. In the ventral striatum’s nucleus accumbens, dopamine serves as a reinforcement signal that helps cement behavioral associations during habit formation. When you encounter an unexpected outcome, like a trove of fresh blueberries on your walking route, your nucleus accumbens receives a dopaminergic signal. This might help you learn to take more walks in this area, which, in the grand scheme of human evolution, is pretty darn helpful. In our modern environment, this can be less adaptive. For example, encountering an unexpectedly cute puppy video on Instagram every 1 in 10 times you open the app might be enough to keep you scrolling, even if you don’t actually enjoy it. Dr. Marianna Pogosyan provides an excellent explanation of the role of dopamine in a Psychology Today article.
So how do dopamine and the reward pathway fit into the biology of ADHD?
The circuit between the prefrontal cortex and the ventral striatum is considered critical for developing habitual behaviors. Dr. Andreas Ströhle and colleagues found that adults with ADHD exhibit less activity in their ventral striatum during the anticipation of delayed rewards than their neurotypical peers. According to one theory, this lower level of baseline reward signaling in the ventral striatum could motivate folks with ADHD to compensate by seeking more immediate gratification. Students with these kinds of brain differences might find it more difficult than their classmates to wait to be called on or to sit through a lecture on something they already know—especially when they might find a more immediate reward in reading a book under their desk. Adults with these differences might find it almost impossible to make it through washing that stack of dishes and instead gravitate towards those potentially cute puppy videos.
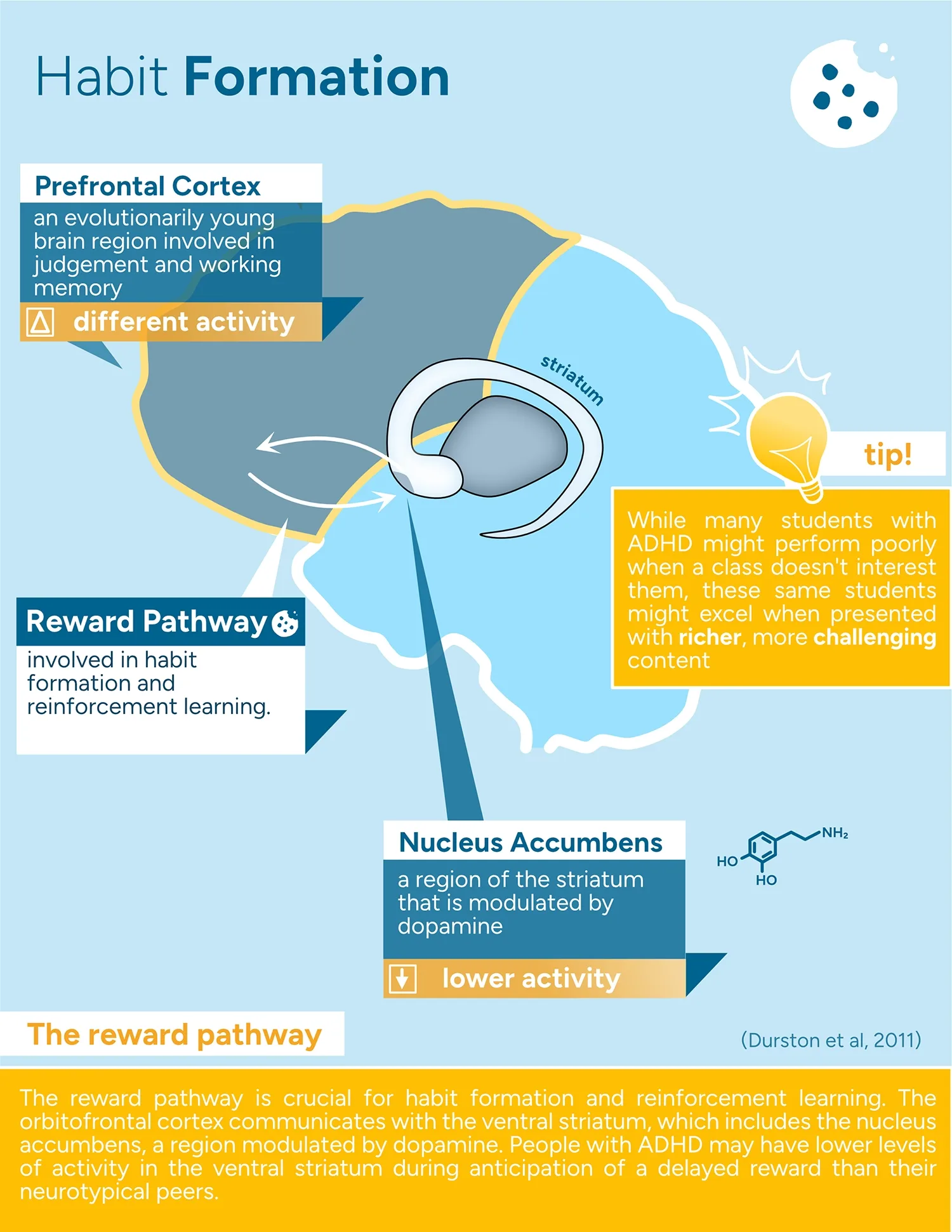
Key takeaway: Habits are solidified through dopamine signaling in the ventral striatum, another brain structure which communicates with the prefrontal cortex. Several studies have found evidence of altered ventral striatal activity in those with ADHD.
The Frontocerebellar Circuit
The cerebellum, or little brain, is a small portion of the hindbrain that accounts for over half of the neurons in the human brain, but only 10% of its volume. This region is crucial for being able to predict outcomes and continuously evaluate and readjust. Classically, the cerebellum has been studied in the context of its role in producing coordinated, adaptive, and practiced movements, but more recently, scientists have begun to explore whether the cerebellum’s ability to predict and evaluate outcomes is used for more than just motor control.
Connections from the cerebellum to the prefrontal cortex via the thalamus may be involved in estimating timing, something which can be a challenge for many with ADHD. Individuals with ADHD often have slight reductions in the size of their cerebella, and may also have reduced functional connectivity between their cerebella and frontal cortices.
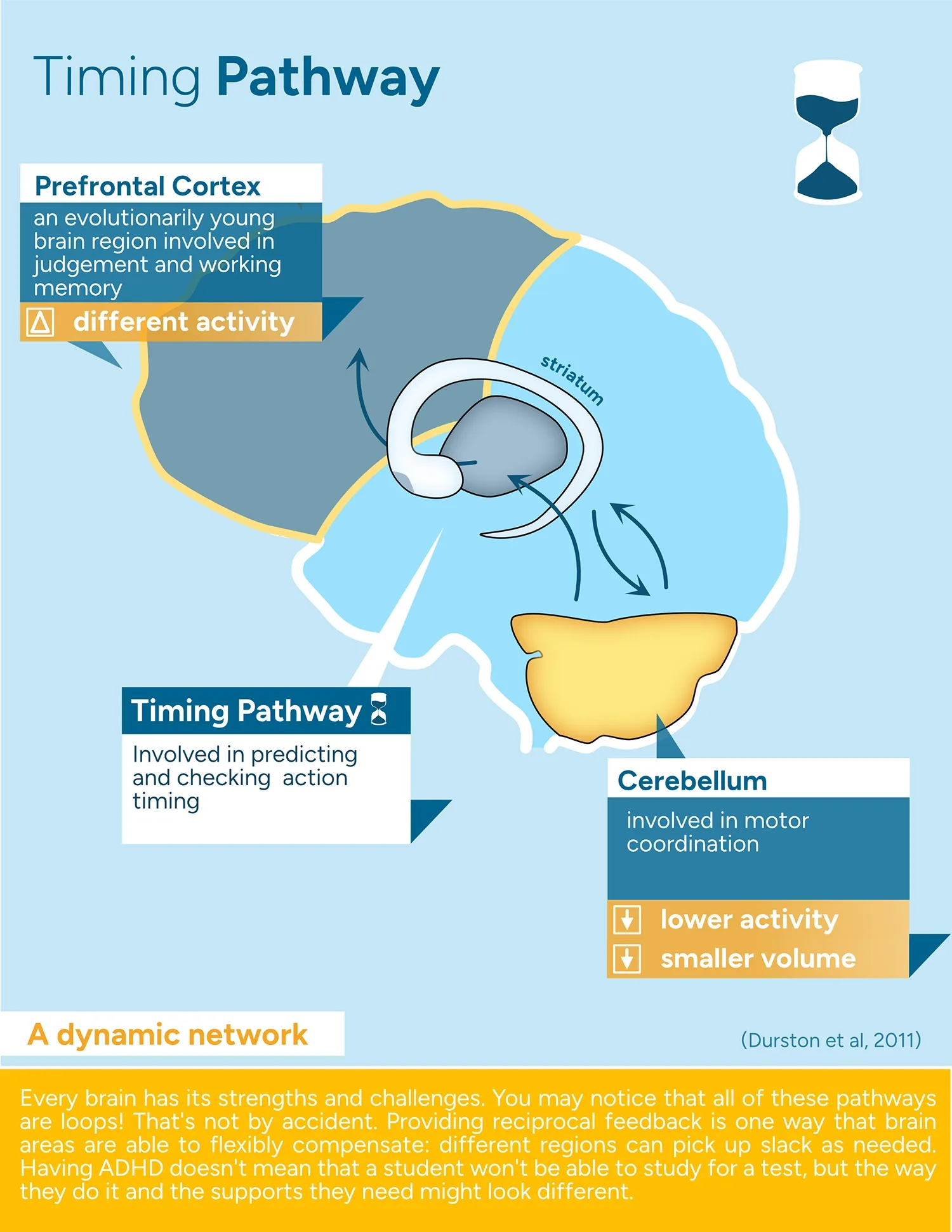
Key takeaway: Connectivity between the cerebellum and the prefrontal cortex may be important for estimating time. It’s possible that differences in cerebellar size and connectivity could underly differences in time estimation between neurotypical folks and those with ADHD.
Putting Circuits into Context
The changes that have been documented in human imaging studies are just a limited snapshot of what’s happening in the brain. This complex organ is constantly adapting and compensating, so lower activity in one region could lead to stronger and more reliable connections to that region. Similarly, weakening of one pathway in the brain can cause alternative pathways to be strengthened.
While the reality of ADHD’s biological basis is indisputable, framing it is something of a balancing act. Biological explanations offer a reprieve from dominant narratives of ADHD as a personal failing or as related to a lack of willpower. But at the same time, overemphasizing biological factors risks framing ADHD as a tragic and incurable illness and promoting fixed mindsets as to what students with ADHD can achieve.
The differences that have been documented between ADHD and neurotypical brains aren’t inherently detrimental or beneficial. Subtle differences in activity, volume, and microstructure can be a boon or a hindrance, depending on the type of activity and the nature of the task at hand.
And herein lies the stickiest point made by the ADHD diagnosis skeptics: that ADHD has been over-pathologized. After all, in an ideal classroom setting, where all students can receive flexible supports that capitalize on their areas of strength, where assessments are well designed to measure learning, and where the content is inherently engaging, ADHD would not impose any barriers to student achievement. Unfortunately, this prospect remains a remote possibility at the moment. And while we shouldn’t need to categorize a human as “broken” to justify their receipt of support services, that is the current legal reality.
So much of the urgency embedded in arguments of an “overdiagnosis epidemic” relies on the idea that accommodations for one student mean that another student loses out. This false-scarcity framing obscures decades of underfunding of disability services. Packaged in new rhetoric, restricting access to accommodations is an old workaround to avoid addressing a systemic issue.
Why Does it Matter?
The dangerous thing about public outcry over overdiagnosis and overtreatment is that it will inevitably lead to students with ADHD being overlooked and undiagnosed. Diagnoses come with options for support in the form of medication, behavioral therapy, and accommodations, should students or families choose to pursue them. So many students with ADHD are already being told some version of “try harder” with the implication that if they were less lazy, they would be able to succeed in school. The truth is that many of these students are working twice as hard as their peers, all while contending with the added burden of outside perceptions that they are unmotivated, flaky, or careless. Biogenic explanations might ease the blame placed on these students, but if they’re not framed appropriately, they can easily become one more lens through which armchair “experts” reduce the reality of neurodivergent students to talking points in a culture war.